
Non-pharmacological analgesia in children and babies beyond the neonatal age
Alfredo Chiurazzi, Andrea Francioni, Neri Demarcus, Carlo V. Bellieni*
Department of Pediatrics, University of Siena, Siena, Italy
Abstract
Introduction: Pain is a major problem in clinical management of children. Pharmacological analgesia is the most commonly used analgesic treatment, but in some cases the use of non-pharmacological analgesic treatments (N-PAT) has been proposed.
Purpose: Our aims were to review the effectiveness and safety of N-PAT for pain relief in children, and to point out which are the most effective.
Material and Methods: We retrieved the clinical trials published in the years 2017-2022 in two databases: PubMed and Index Medicus, analyzing them with the PRISMA method. We used the following key-words: distraction, pain, child. Then we refined our search using in the same databases the key-words “pain” and “child”, matched with the terms that describe the N-PAT: “Virtual reality”, “Robot”, “Audiovisual distraction”, “Audio Distraction”, “Buzzy”, “Videogames”, “Parents verbal interactions”, “Distraction cards”, “Magic glove”, “Ipad”, “Picture book”, “Kaleidoscope”, “Soap bubbles” and “Hand massage”. Exclusion criteria were: reviews, case reports, papers in a language other than English, including patients other than children older than one month of age.
Results: We have screened 126 articles and 66 were excluded from the final pool. The most studied painful stimulation was needle procedures, where the most effective N-PAT was virtual reality, followed by the buzzy system. In the case of other painful procedures, few studies were available; however, in any of these painful stimulations effective analgesia was obtained with the use of virtual reality. Several studies eventually show that the combination of N-PAT with analgesic topic drugs provides more effective analgesia.
Conclusion: Some non-pharmacological treatments appear actually effective. The research in this field should be implemented to get more conclusive data, but our results are in favor of more extended use of N-PAT during potentially painful procedures.
Introduction
Pain is an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage1.
Children may be exposed to painful interventions for the purpose of diagnosis, or treatment2. The painful interventions most commonly performed in children include phlebotomy, injection, and vaccination. During these interventions, it is highly important to use methods that have a pain relieving effect3. Pharmacologic and non-pharmacologic analgesic treatments (N-PAT) can be used separately or together to reduce the pain during invasive procedures4. Studies of both pharmacologic and N-PAT in procedural pain relief determined that N-PAT were as effective as pharmacologic methods4,5,6. N-PAT can be preferred in relieving procedural pain, because pharmacologic methods can have side effects7, but also because several studies support the effectiveness of N-PAT in managing the pain associated with invasive procedures in children8,9,10. Moreover, the non-pharmacological approach to pain prevention is important in the vision of a humanized treatment of the young patient, who needs to find a welcoming and non-stressing environment, under the condition that interventions used for optimal pain management should be effective, reliable, child-friendly, and hopefully should not extend the procedure time11.
Several studies have been performed in the neonatal period to evaluate the efficacy of N-PAT12,13,14, but much less in the postnatal period. For this reason, we felt that an updated review of the state of the art on N-PAT (Table 1) in older children was important.
Table 1: The 5 most used non-pharmacological analgesia techniques with definition
|
VIRTUAL REALITY |
Simulated experience of real or ureal situations lived through an external device (VR glasses, VR headsets) |
|
BUZZY DEVICE |
Handheld device about the size of a computer mouse that buzzes (vibrates) on the skin |
|
AUDIOVISUAL DISTRACTION |
Passive distraction like watching television or video with the phone |
|
VIDEOGAMES |
Active audio-visual distraction like PlayStation |
|
PARENTAL VERBAL INTERACTION |
Mother/father speaking and cuddling the child during procedures. |
Study Purpose
The purpose of this article is to provide a critical assessment of the evidence-based literature on N-PAT in pediatric age.
Materials and Methods
We retrieved the clinical trials published in the years 2017-2022 in two databases: PubMed and Index Medicus. In the first phase of our search, we used the following key-words: distraction, pain, child. To make our search more complete, in the second phase we searched papers in the same databases using the key-words “pain” and “child”, but matching them with each of the following terms that describe the most used N-PAT: “Virtual reality”, “Robot”, “Audiovisual distraction”, “Audio Distraction”, “Buzzy”, “Videogames”, “Parents verbal interactions”, “Distraction cards”, “Magic glove”, “Ipad”, “Picture book”, “Kaleidoscope”, “Soap bubbles” and “Hand massage”.
Inclusion criteria were: dealing with children with postnatal age ranging 1 month-17 years; use of a validated pain scale to assess pain; availability of raw data of pain reported by the children during the painful procedure; articles in English; fully available statistical data. We screened the whole pool of papers using the PRISMA criterion (Table 2).
Table 2: Studies included in the analysis
|
First Author, year |
Population |
Setting |
Intervention |
Other intervention |
Primary outcome |
p-value |
|
|
Intervention |
control |
||||||
|
15 Shetty V, 2019
|
N= 118 (5-8 year old) |
Group 1 |
VR |
N/A |
SCL: pre 83.45 (12.03) ng/ml intra 68.45 (13.03) ng/ml post 62.55 (13.28) ng/ml
WBFPS mean and median: 2.42 (1.47), 2 (0.52)
|
SCLcontrol: pre 78.35 (14.13) ng/ml, intra 70.72 (13.65) ng/ml, post 62.13 (13.83) ng/ml
WBFPS control: 5.6 (1.22), 6 (4,6)
|
SCL pre-intra: p<0.001 Intra-post: p<0.001 Post-intra: p<0.001
WBFRPS: <0.001
|
|
43 Gamze Inan, 2019
|
N= 180 (6-10) |
Group 2
|
AVD |
VG PVI |
WBFPS: AVD: 3.02 ± 2.94 VG: 1.42 ± 1.74 PVI: 2.89 ± 3.00
|
WBFPRS control: 5.11 ± 3.78
|
VG vs AVD and PVI: p<0.05
VG/AVD/PVI vs control: p<0.01
AVD vs PVI: ns
|
|
16 BirguÌl Erdogan, 2021
|
N= 142 (7-12) |
Group 2
|
DC
|
VR B |
WBFPS B: 0.9 ± 0.9 VR: 0.9 ± 0.9 DC: 1.4 ± 1.2
VAS B: 2.2 ± 2.0 VR: 2.7 ± 2.8 DC: 3.4 ± 2.4
|
WBFPS control: 2.5 ± 1.7
VAS control: 5.2 ± 2.8
|
WBFPS DC vs control: p<0.05 VR vs control: p<0.01 B: vs control: p<0.01 DC vs B, VR vs B e VR: DC: ns
VAS: DC vs control: p<0.05 VR vs control: p<0.01 B: vs control: p<0.01 DC vs B, VR vs B e VR: DC: ns
|
|
50 Volkan Susam 2018
|
N= 64 (3-10) |
Group 2 |
B + DC |
MG |
Integration WBFPS, VAS and NRS:
B+DC: 3.66±2.02
MG: 4.74±2.07
|
N/A
|
p=0.039 |
|
17 Søren Walther-Larsen 2019
|
N=59 (7-16) |
Group 2
|
VR |
N/A |
VAS: 27 (8 to 33)
|
VAS control (standard of care): 15 (5 to 30)
|
p=0.23 |
|
45 N.C.A.C. Oliveira, 2017
|
N= 40 (6-11) |
Group 2
|
AVD: G1 T1: 22 G2 T2: 18 |
N/A |
WBFPS G1 T1: 1.91 +/- 1.68 G2 T2: 2.67 +/- 2.74
VAS G1 T1: 1.50 +/- 1.87 G2 T2: 2.33 +/- 2.54
|
WBFPS control: G1 T2: 3.64 +/- 3.06 G2 T1: 6.78 +/- 3.15
VAS control: G1 T2: 3.32 +/- 3.42 G2 T1: 6.28 +/- 2.86
|
AVD vs control: p<0.01 |
|
18 GuÌlçin OÌzalp Gerçeker 2021
|
N= 42 (6-17) |
Group 2
|
VR |
N/A |
WBFPS: 2.4 ± 1.8
|
WBFPS control: 5.3 ± 1.8
|
p<0,01 |
|
19 Yen-yu Chen 2020
|
N= 136 (7-12) |
Group 2 |
VR |
N/A |
WBFPS: 3.35±2.38 |
WBFPS control: 4.35±2.95 |
p=0.031 |
|
70 Zoe Grabinski, 2022
|
N= 40 |
Group 2 |
Distarction |
N/A |
WBFPS 1.4; 95% CI, 0.9-1.9
|
WBFPS 1.3, 95% CI, 0.5-2.1
|
ns |
|
68 Sherwood Burns-Nader 2017
|
N= 30 (4-12) |
Group 3
|
IPad |
N/A |
WBFPS: 2.53 (1.64)
|
WBFPS control: 3.20 (1.78)
|
p=0.29
|
|
20 Osama M. Felemban, 2021
|
N=50 (6-12) |
Group 1
|
VR |
AVD |
FLACC: VR: 2.58 ± 1.99 AVD: 2.18 ± 2.29 WBFPS: VR: 2.40 ± 2.82 AVD: 2.72 ± 2.99 |
N/A
|
p=0.497 p=0.707 |
|
41 Samina Ali, 2021
|
N: 81 (6-11) |
Group 2
|
R |
N/A |
OSBD-R: 0.78 ± 1.32
WBFPRS: 2 (0, 4)
|
OSBD-R control: 1.49 ± 2.36
WBFPS control: 4 (2,6)
|
p<0.05 p<0.13 |
|
67 Remziye Semerci, 2020
|
N=90 (6-12) |
Group 2
|
DC K |
N/A |
VAS: DC: 2.32 ± 2.55 K: 2.72 ± 3.29
|
VAS control: 6.24 ± 3.93
|
DC vs control: p<0.001 K vs control: p<0.001 DC vs K: p<0.938
|
|
51 Sevil Inal, 2020
|
N=218 (6-12) |
Group 2
|
DC |
B DC + B |
WBFPS: B: 1.38 ± 1.3 DC: 2.43 ± 1.3 DC+B: 0.53 ± 0.9
|
WBFPS control: 4.46 ± 2.9
|
DC/B/DC+B vs control: p<0.001 |
|
21 Henry Xiang, 2021
|
N: 90 |
Group 3
|
VR
|
AVD |
VAS: IVR: 24.9 [95% CI, 12.2- 37.6]
|
VAS control: 47.1 [95% CI, 32.1-62.2]
|
IVR vs control: p=0.02
|
|
44 F. Guinot , 2021
|
N= 68 |
Group 1
|
VG
|
PVR (AVD) |
WBFPS: IVR: 0±0.26
|
WBFPS: PVR: 0.94±1.41
|
p=0.013
|
|
71 Aylin Arıkan, 2020
|
N=216 (6-12) |
Group 2
|
ID
|
PD |
WBFPS: ID: 2.60 (1.54) PD: 2.60 (1.54)
VAS: ID: 1.50 (0.65) PD: 1.97 (0.81) |
WBFPS control: 7.33 (2.41)
VAS control: 3.79 (1.08)
|
WBFPS: control> PD > ID: p < 0.001
VAS: control>PD>ID: p<0.001
|
|
22 Fadime Ustuner , 2021 |
N: 77 |
Group 2 |
VR |
N/A |
WBFPS: 3.82 ± 1.20 |
WBFPS: 6.96 ± 2.08
|
p=0.0001 |
|
52 Cozzi, 2018 |
4-12y (n=200) |
Group 2 |
B |
T |
Faces pain scale-revised (4-7y) Numerical rating scale (8-12y) median (IQR): B: 3 (1-4.8) T: 2 (1-4.8) |
N/A |
B vs. T: p=0.72 |
|
23 Le May, 2020 |
7-17y (n=20) |
Group 3 |
VR |
N/A |
Numerical rating scale of pain (0-10) mean±SD: 3.8±3.4 |
control: 4.8±3.1 |
p=0.023 |
|
10 Risaw, 2017 |
4-6y (n=210) |
Group 2 |
DC |
N/A |
FLACC mean±SD: DC: 2.75±0.97 |
control: 3.24±0.85 |
p<0.001 |
|
53 Redfern, 2018 |
3-18y (n=50) |
Group 2 |
B |
N/A |
WBFS mean±SD: B: 3.56±3.2 |
control: 5.92±3.4 |
p=0.015 |
|
24 Alshatrat, 2021 |
5-12y (n=54) |
Group 1 |
VR + local anesthesia |
N/A |
FLACC mean (SD): VR+local anesthesia: 2.588±3.001 |
control (local anesthesia): 5.571±3.857 |
p=0.0132 |
|
25 Custòdio, 2020 |
6-9y (n=44) |
Group 1 |
VR +local anesthesia |
N/A |
Venham Scale mean (SD): AVE+local anesthesia: 0.41 (1.53) |
control (local anesthesia): 1.32 (1.92) |
p=0.07 |
|
69 Kuo, 2018 |
3-7y (n=276) |
Group 2 |
PB |
iPad |
OSBD-R mean (SD): PB: 27.4 (5.6) Cartoons in iPad: 28.9 (6.3) |
control (routine oral instructions): 38.5 (14.6) |
PB vs. control: p<0.001 iPad vs. control: p<0.001 PB vs. iPad: ns
|
|
26 Osmanlliu, 2021 |
7-17y (n=62) |
Group 2 |
VR+standard of care |
N/A |
Verbal numerical rating scale (0-10) median (IQR): 3 (1-6) |
control (standard of care): 3 (1-5.5) |
p=0,75 |
|
46 van der Heijden, 2019 |
3-13y (n=191) |
Group 2 |
AD |
AVD |
AHTPS mean (SD): AD: 2 (2.05) AVD: 2.86 (2.62) |
control (standard of care): 3.10 (2.24) |
AD vs. control: p=0.006 AVD vs. control: p=0.328 |
|
27 Semerci, 2020 |
7-18y (n=71) |
Group 2 |
VR |
N/A |
WBFS mean±SD: VR: 2.34±3.27 |
control: 5.02±3.35 |
p=0.001 |
|
28 Liu, 2020 |
7-17y (n=53) |
Group 4 |
VR |
N/A |
WBFS mean±SD: 0.80±1.06 |
control (standard of care): 2.26±2.38 |
p=0.018 |
|
29 Buyuk, 2021 |
5-10y (78) |
Group 5 |
VR |
N/A |
WBFS mean±SD: VR: 1.35±1.09 |
control: 3.00±1.52 |
p<0.01 |
|
30 Ran, 2021 |
4-8y (n=120) |
Group 1 |
VR |
N/A |
WBFS mean±SD: VR: 1.62±1.13 |
control (Tell-show-do): 3.59±1.19 |
p<0.001 |
|
66 Erdogan, 2019 |
1-3y (n=60) |
Group 2 |
PVI |
N/A |
FLACC mean±SD: PVI: 4.76±2.43 |
control: 7.66±3.75 |
p=0.000 |
|
31 Jeffrey I. Gold,2021 |
10-21 y (n=107) |
Group 2 |
VR |
N/A |
Faces pain scale-revised mean (SD): 1.09 (1.82) |
2.19 (2.21) |
p=0.002 |
|
32 Tuba Koc Ozkan, 2019 |
4-10 y (n=139) |
Group2 |
VR |
K |
WBFS mean±SD: VR: (1.76+1.4) K: (2.76+1.8) |
6.65+2.2 |
K vs control: p<.000 VRvs control: p<.000 VR vs K: p=0.039 |
|
47 Fatemeh Cheraghi, 2021 |
6-12 y (n=120) |
Group 3 |
AD |
AVD |
Ocher Pain Scale: mean±SD: AD:3.97 ±12.13 VD: 3.86 ±12.28 |
4.08±12.42 |
AVD vs control: p<0.001 AD vs control: p<0.001 AVD vs AD: p=0.004 |
|
33 Demet Ä°nangil,2020 |
3-18 y (n=120) |
Group 2 |
VR |
Tablet |
WBFS: mean±SD: VR box: 1.3±2.15 Tablet: 4.55±3.44 |
4.95±3.65 |
p<0.001 |
|
65 Xiu-Hang Zhang, 2020 |
1-3y (n=120) |
Group 3 |
Medical screen |
VG |
MBPS: mean (SD): Medical screen: 6.78(0.82) VG: 7.775(0.80)
|
8.45(0.51) |
p<0.001 |
|
72 Xiu-Hang Zhang, 2020 |
1-3y (n=52) |
Group 3 |
Medical screen |
N/A |
MBPS: mean (SD): Medical screen: 6.77 (1.42) |
8.50 (0.51) |
p<0.001 |
|
54 Seyda Binay, 2018 |
3-6y (n=96) |
Group 2 |
B |
SB |
WBFS mean±SD: ECV: 3.12±0.38 BSB: 2.15±0.35 |
7.37±0.38 |
B vs SB: p=0,387 B/SB versus control: p<.000 |
|
48 J.-S. Song, 2020 |
3-7y (n=48) |
Group 3 |
AVD |
N/A |
WBFS mean (SD): 6 (22.43) |
0 (15.66) |
p<0,001 |
|
49 Muhammet Bulut, 2020 |
7-11 y (n=140)
|
Group 5 |
AD |
K HM |
WBFS mean (SD): AD: 1.68 (1.13) K: 1.08 (0.98) HM: 1.31 (1.10) |
2.45 (0.95) |
p=0,000 |
|
34 Jordan S. Taylor |
6-17 y (n=70) |
Group 5 |
VR |
N/A |
Verbal Pain Scale mean±SD: VR: 0.4 ±1.1 |
0.03± 0.2 |
p=0.073 |
|
35 A. Garrocho-Rangel |
5-8 y
|
Group 1 |
VR |
N/A |
FLACC mean (SD): VEES 1.03 (2.21) |
0.64 (1.31) |
p=0.7 |
|
56 Yilmaz, 2020 |
8-16y (n=60) |
Group 2 |
B |
N/A |
FACES mean (SD): B: 1.36 (1.12) |
control: 1.33 (1.15) |
p=0.829 |
|
57 Bourdier, 2021 |
18m-6y (n=607) |
Group 2 |
B |
N/A |
Children's Hospital of Eastern Ontario Pain Scale mean (SD): B: 8.5 (2.6) |
EMLA patch: 7.2 (2.4) |
EMLA patch vs B: p<0.01 |
|
58 Bilgen, 2019 |
7-12y (n=150) |
Group 2 |
B |
ShotBlocker |
FACES mean (SD): B: 3.64 (3.10) ShotBlocker: 6.24 (3.20) |
control: 7.36 (3.09) |
B vs control: p<0.01 B vs ShotBlocker: p<0.01 |
|
59 Sahiner, 2018 |
6-12y (n=60) |
Group 2 |
B |
ShotBlocker |
FACES mean (SD): B: 1.26 (1.36) ShotBlocker: 0.9 (1.20) |
control: 3.2 (2.78) |
p=0.008 |
|
60 Alemdar, 2019 |
5-10y (n=195) |
Group 2 |
B |
SB Aromatherapy |
Oucher pain scale mean (SD): B: 3.51 (3.49) SB: 4.53 (3.25) Aromatherapy: 5.46 (2.75) |
control: 5.87 (2.87) |
B vs control: p<0.05 |
|
61 Ueki, 2020 |
0-6y (n=118) |
Group 2 |
B |
N/A |
FLACC mean (SD): BD: 6.98 (3.28) |
control: 7.63 (2.79) |
p=0.25 |
|
42 Lee-Krueger, 2021 |
4-12y (n=137) |
Group 2 |
R |
N/A |
Faces Pain Scale-Revised mean±SD: MEDi Robot: 2.74 (2.96) |
control: 2.76 (2.97) |
p=0.98 |
|
55 Yilmaz, 2019 |
5-10y (n=120) |
Group 2 |
B |
ShotBlocker SB |
Oucher pain scale mean (SD): B: 3.87 (1.79) ShotBlocker: 4.14 (2.12) SB: 4.75 (1.74) |
control: 6.72 (2.16) |
ShotBlocker vs Control: p<0.05 B vs Control: p<0.05 SB vs Control: p<0.05 |
|
62 Sapci, 2021 |
3-18y (n=90) |
Group 2 |
B |
N/A |
FACES mean (SD): B: 2.44 (1.85) |
control: 5.77 (2.14) |
p<0.05 |
|
36 Gerceker 2018 |
7-12 y (n = 121) |
Group 2 |
VR |
B |
WBFPS mean (SD): VR: 1.5 (0.2) B: 2 (0.2) |
control: 5.1 (0.4) |
VR vs control: p<0.05 B vs control: p<0.05 |
|
63 Alanazi 2018 |
6-7 y (n = 60) |
Group 1 |
B + Analgesia |
Analgesia |
WBFPS mean rank (sum of ranks) B + analgesia: 17.50 (1759.00) Analgesia: 3.50 (10.50) |
N/A |
WBFPS p <0.001
|
|
64 Bilisin 2019 |
n = 60 |
Group 1 |
B + Analgesia |
Analgesia |
WBFPS mean (SD) B + analgesia: 0.867 (1.136) Analgesia: 3.333 (1.917) |
N/A |
p<0.01 |
|
37 Eijlers R.
|
4-12 y (n=200) |
Group 5 |
VR |
N/A |
FPS-r: VR: 2.0 [0.0 to 4.0]
|
2.0 [0.0 to 2.5]
|
p=0.699
|
|
117 Özalp Gerçeker G
|
5-12 y (136) |
Group 2 |
VR-Rollercoaster
|
VR-Ocean Rift
|
WBFS mean ± (SD) (min-max): VR-Rollercoaster=1.2 ± 2.2 (0-10) VR-Ocean Rift= 1.0 ± 1.5 (0-6)
|
4.1 ± 3.5 (0-10)
|
p=0.000
|
|
38 Aydın Aİ
|
(n=120) |
Group 2 |
VR |
N/A |
WBFS mean ± (SD) VR: 1.68 ± 1.51
|
2.02±1.96
|
p=0.006
|
|
39 Tennant M
|
7-19 y (n=90) |
Group 6 |
VR
|
IPad |
VAS mean (SD): VR 10.97 (11.23) IPad 12.82 (11.34) |
N/A |
p=0.475
|
|
40 Arman N |
6-18 (n=62) |
Group 6 |
VR |
TOAT |
NRS mean (SD): VR: 0.64 (1.31) TOAT: 1.04 (1.62) |
N/A |
p=0.000 |
Legend: R: Robot, VR: virtual reality, AVD: audio-visual distraction, AD: audio distraction, B: Buzzy system, DC: Distraction Cards, K: Kaleidoscopic, T: tablets, VG: videogames, PVI: parents verbal interaction, SB: soap bubbles, MG: Magic Glove, HM: hand massage, WBFPS: wong baker faces pain rating scale, SCL: salivary cortisol levels, VAS visual analogue scale, NRS numeric rating scale, Others (ID: interactive distraction, PD: passive distraction, TOET, medical screen), OSBD-R: Observed Scale of Behavioral Distress-Revised; CFS: Children's Fear Scale MBPS: modified behavioural pain scale, FLACC: Face Legs Activity Cry Consolability, AHTPS: Alder Hey Triage Pain Score, ns: not significant, CI: confidence intervals
Group 1: Dental treatment, Group 2: Needle related procedures, Group 3: Medical procedures in children with burns, Group 4: Endoscopic procedures, Group 5: Surgery procedures, Group 6: Oncology and rheumatology disease therapy
Results
We found in total 197 articles of which 83 were found during the first search on databases and 114 during the second part; 71 were removed during the second search, because they were duplicates of the first research. Out of these 126 articles, 65 were excluded for reporting data on pain in newborn and adult (n=6), data not on pain (n=27), incomplete statistical data (n=11), non-English written articles (n=3), pilot studies (n=8), too small sample of babies (n=1), inability to retrieve the full text of the paper (n=10). A total of 61 articles were included in this review75-116 (Table 2).
The included articles described the following non-pharmacological analgesia techniques: Virtual reality (n=27)15-40, Robot (n=2)41,42, Audio visual distraction (n=8)21,43-48, Audio distraction (n=3)46,47,49, Buzzy (n=17)16,36,50-64, Videogames (n=3)43,44,65, Parents verbal interactions (n=2)43,66, Distraction cards (n=5)10,16,50,51,67, Magic glove (n=1)50, IPad (n=5)33,39,52,68,69, Picture book (n=1)69, Kaleidoscope (n=3)32,49,67, Soap bubbles (n=1)54, Hand massage (n=1)49 (Table 3). The data on how many times the method used was significant in a given setting can be found in Table 4. Out of the 61 selected studies15-74, 40 concern needle related procedures16-19,22,26,27,31,32,36,38,41-43,45,46,50-62,66,67,69,71,117, 8 dental treatment15,20,24,25,30,35,44,64, 6 medical procedures in children with burns21,23,47,65,68,72, 4 surgery procedures29,34,37,49, 1 endoscopic procedures28 and 2 oncology and rheumatology disease39,40.
Table 3: Studies screened from PubMed database
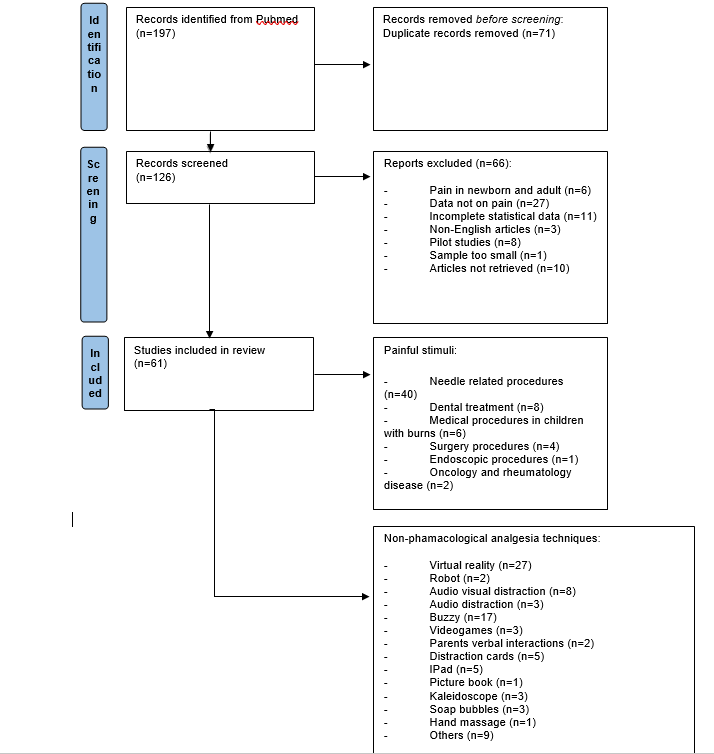
Table 4: Comparisons of non-pharmacological methods vs Standard of care
|
Technique vs Control |
Needle related procedures |
Dental treatment |
Medical procedures in children with burns |
Surgery procedures |
Endoscopic procedures |
Oncology and rheumatology disease |
|
Virtual reality |
S=12 (vs Control) NS=2 (vs Control) |
S=4 (vs Control) NS=1 (vs Control) |
S=2 (vs Control) |
S=2 (vs Control) NS=1 (vs Control) |
S=1 (vs Control) |
|
|
Robot |
NS=2 (vs Control) |
|
|
|
|
|
|
Audio visual distraction |
S=2 (vs Control) NS= 2 (vs Control)* |
|
S=2 (vs Control) NS=1 (vs Control) |
|
|
|
|
Buzzy |
S=10 (vs Control) NS=2 (vs Control) |
S=2 (vs Control)
|
|
|
|
|
|
Videogames |
S=1 (vs Control) |
|
S=1 (vs Control) |
|
|
|
|
Parents verbal interactions |
S=2 (vs Control) |
|
|
|
|
|
|
Distraction cards |
S=4 (vs Control) |
|
|
|
|
|
|
Magic glove |
|
|
|
|
|
|
|
IPad |
S=2 (vs Control) |
|
NS=1 (vs Control) |
|
|
|
|
Picture book |
S=1 (vs Control) |
|
|
|
|
|
|
Kaleidoscope |
S=2 (vs Control) |
|
|
S=1 (vs Control) |
|
|
|
Soap bubbles |
S=2 (vs Control) NS=1 (vs Control) |
|
|
|
|
|
|
Hand massage |
|
|
|
S=1 (vs Control) |
|
|
|
Audio distraction |
S=1 (vs Control) |
|
S=1 (vs Control)
|
S=1 (vs Control)
|
|
|
|
Others |
S= 3 (vs Control) NS=1 (vs Control) |
|
S= 2 (vs Control)
|
|
|
|
S: Treatment group is significantly better than control; NS: No significant difference
Here we report the results for each painful procedure.
Needle related procedures: The most effective N-PAT were the virtual reality in 12 studies16,18,19,22,27,31,32,36,38,117, in 2 studies it was the audiovisual distraction43,45, in 10 the buzzy system16,36,53-55,57-60,62, in 4 the distraction cards10,16,51,67, in 1 the picture books69, in 2 the kaleidoscope32,67, in 2 the soap bubbles54,55, in 1 the videogames43, in 2 the parental verbal interactions43,66, in 1 the combination of distraction cards with the buzzy system50, in 1 the audio distraction46 and in 1 the iPad68,69. In no study the robots, magic glove and hand massage were effective.
Dental treatment: The most effective N-PAT was the virtual reality in 4 study15,24,25,30, in 2 studies it was the buzzy system63,64 and in no study the robots, audiovisual distraction, videogames, parents verbal interactions, distraction cards, magic glove, iPad, picture book, kaleidoscope, soap bubbles, hand massage and the combination of distraction cards with buzzy system.
Procedures in children with burns: The most effective N-PAT was the virtual reality21,23in 2 studies, in 2 studies the audiovisual distraction21,47, in 2 studies others techniques (medical screen)65,67, in 1 study videogames65, in 1 study audio distraction47 and in no study the robots, buzzy system, , parents verbal interactions, distraction cards, magic glove, iPad, picture book, kaleidoscope, soap bubbles, hand massage and the combination of distraction cards with buzzy system.
Surgical procedures (circumcision, hormone implant placement): The most effective N-PAT was the virtual reality in 2 studies29,34, in 1 study it was the audiovisual distraction49, in 1 study the kaleidoscope49, in 1 study the hand massage49 and in no study the robots, buzzy system, videogames, parents verbal interactions, distraction cards, magic glove, iPad, picture book, soap bubbles and the combination of distraction cards with buzzy system.
Endoscopic procedures: The most effective N-PAT was the virtual reality in 1 study28 and in no study the robots, audiovisual distraction, buzzy system, videogames, parents verbal interactions, distraction cards, magic glove, IPad, picture book, kaleidoscope, soap bubbles, hand massage and the combination of distraction cards with buzzy system.
Procedures correlated to oncology and rheumatology diseases: The most effective N-PAT were the videogames40 in 1 study and in no study the virtual reality, robots, audiovisual distraction, buzzy system, parents verbal interactions, distractions cards, magic glove, iPad, picture book, kaleidoscope, soap bubbles, hand massage and the combination of distraction cards with buzzy system.
When comparing N-PAT with pharmacological analgesia techniques, one study57 showed the superiority of the EMLA gel over the use of the buzzy device. Two studies63,64 showed the superiority of the combined use of buzzy device and analgesia with lidocaine compared to the use of only lidocaine. Two studies24,25 showed the superiority of the combined use of virtual reality and local analgesia compared to the use of only local analgesics.
As for the effectiveness of NPATs based on the age of children, it seems that virtual reality is more effective in children between the ages of 7 and 12 (average age 10.8 years)15-40. While with regard to buzzy devices, the age at which these systems are most effective is between 7 and 10 years (average age 8.9 years)16,36,50-64,117-121. Unfortunately, the few published studies regarding the other techniques used do not allow to detect an evident efficacy on a certain age range of the tested children.
Discussion
This review analyzed the clinical trials conducted between 2017 and 2022 and examined which are the most effective non-pharmacological analgesic techniques in the treatment of pediatric pain. The articles analyzed compared specific N-PAT with controls.
Our search showed that virtual reality was the most often used N-PAT, moreover it appears to be the most effective compared vs control in particular in the field of venipuncture. The buzzy device system was the second most used technique. Scarce studies were developed in this period using other N-PAT (Robot, Audio visual distraction, Video Games, Parents verbal interactions, Distraction cards, Magic glove, IPad, Picture book, Kaleidoscope, Soap bubbles, Hand massage).
The use of N-PAT is important to avoid pain in children2. Stress and pain are factors that can alter a child's homeostasis, causing fear, increased blood pressure and tachycardia122. They can also cause the child's lack of compliance with the pediatrician and nurse, as well as make him lose confidence in them during future visits. The relationship with the healthcare environment must avoid being traumatic123.
Unfortunately, children and their families still feel uncomfortable when going to a medical visit: for an ancient equation between visit and pain, saying “no pain no gain” seems always true, and analgesia during procedural pain is still scarcely used, though today we have valid tools to avoid pain as this review has shown. Pain management in pediatrics is still defined as “suboptimal”124, and this has become a “major public health problem”125.
Procedural pain is less painful than surgical or physically traumatic pain, but it cannot be ignored: we know that repeated stress and suffering even has a negative epigenetic effect on the expression of corticosteroid receptor genes or for the brain growth factor; repeated pain causes growth retardation of the cerebral cortex126. This is especially true for hospitalized patients who receive numerous painful events; the physical and psychological risks associated with pain are not absent even when pain is experienced after the first month of life12,14.
In conclusion, despite the need for further studies, this review shows the effectiveness of several N-PAT. There is enough evidence to recommend the use of these methods, particularly in the context of skin punctures. Further studies must be conducted comparing the various N-PAT and their use in combination with drug analgesia.
References
- Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020; 161(9): 1976-1982.
- Koller D, Goldman RD. Distraction techniques for children undergoing procedures: A critical review of pediatric research. J Pediatr Nurs. 2012; 27: 652-681.
- Aydin D, Sahiner NC, Ciftci EK. Comparison of the effectiveness of three different methods in decreasing pain during venipuncture in children: Ball squeezing, balloon inflating and distraction cards. J Clin Nurs. 2016; 25: 2328-2335.
- Bahorski JS, Hauber RP, Hanks C, et al. Mitigating procedural pain during venipuncture in a pediatric population: A randomized factorial study. Int J Nurs Stud. 2015; 52: 1553-1564.
- Boivin JM, Poupon-Lemarquis L, Iraqi W, et al. A multifactorial strategy of pain management is associated with less pain in scheduled vaccination of children. A study realized by family practitioners in 239 children aged 4-12 years old. Fam Pract. 2008; 25: 423-429.
- Russell K, Nicholson R, Naidu R. Reducing the pain of intramuscular benzathine penicillin injections in the rheumatic fever population of Counties Manukau District Health Board. J Paediatr Child Health. 2014; 50: 112-117.
- Jacop E. Pain assessment and management in children. In: Hockenberry M, Wilson D, eds. Wong’s Nursing Care of Infants and Children, 9th ed. St. Louis, MO: Elsevier Mosby. 2011: 179-226.
- Heden L, Von Essen L, Ljungman G. Randomized interventions for needle procedures in children with cancer. Eur J Cancer Care. 2009; 18: 358-363.
- Inal S, Kelleci M. Relief of pain during blood specimen collection in pediatric patients. MCN Am J Matern Nurs. 2012; 37: 339-345.
- Risaw L, Narang K, Thakur JS, et al. Efficacy of Flippits to reduce pain in children during venipuncture—A randomized controlled trial. Indian J Pediatr. 2017; 84: 597-600.
- Cohen LL, MacLaren JE, DeMore M, et al. A randomized controlled trial of vapocoolant for pediatric immunization distress relief. Clin J Pain. 2009; 25: 490-494.
- Mangat AK, Oei JL, Chen K, et al. A Review of Non-Pharmacological Treatments for Pain Management in Newborn Infants. Children. 2018; 5(10): 130. doi: 10.3390/children5100130. PMID: 30241352; PMCID: PMC6210323.
- Theingi S, Leopold I, Ola T, et al. Virtual Reality as a Non-Pharmacological Adjunct to Reduce the Use of Analgesics in Hospitals. J Cogn Enhanc. 2021: 1-6. doi: 10.1007/s41465-021-00212-9. Epub ahead of print. PMID: 33842827; PMCID: PMC8022314.
- Aguilar Cordero MJ, Baena García L, Sánchez López AM, et al. procedimientos no farmacológicos para disminuir el dolor de los neonatos; revisión sistemática [non pharmacological methods to reduce pain in newborns; systematic review]. Nutr Hosp. 2015; 32(6): 2496-507. Spanish. doi: 10.3305/nh.2015.32.6.10070. PMID: 26667696.
- Shetty V, Suresh LR, Hegde AM. Effect of Virtual Reality Distraction on Pain and Anxiety During Dental Treatment in 5 to 8 Year Old Children. J Clin Pediatr Dent. 2019; 43(2): 97-102. doi: 10.17796/1053-4625-43.2.5. Epub 2019 Feb 7.
- Erdogan B, Aytekin Ozdemir A. The Effect of Three Different Methods on Venipuncture Pain and Anxiety in Children: Distraction Cards, Virtual Reality, and Buzzy® (Randomized Controlled Trial). J Pediatr Nurs. 2021; 58: e54-e62. doi: 10.1016/j.pedn.2021.01.001.
- Walther-Larsen S, Petersen T, Friis SM. Immersive Virtual Reality for Pediatric Procedural Pain: A Randomized Clinical Trial. Clin Exp Dent Res. 2021; 7(5): 795-802. doi: 10.1002/cre2.407.
- Gerçeker GÖ, BektaÅ M, Aydınok Y, et al. The effect of virtual reality on pain, fear, and anxiety during access of a port with huber needle in pediatric hematology-oncology patients: Randomized controlled trial. Eur J Oncol Nurs. 2021; 50: 101886. doi: 10.1016/j.ejon.2020.101886. PMID: 33321461.
- Chen YJ, Cheng SF, Lee PC. Distraction using virtual reality for children during intravenous injections in an emergency department: A randomised trial. J Clin Nurs. 2020; 29(3-4): 503-510. doi: 10.1111/jocn.15088.
- Felemban OM, Alshamrani RM, Aljeddawi DH. Effect of virtual reality distraction on pain and anxiety during infiltration anesthesia in pediatric patients: a randomized clinical trial. BMC Oral Health. 2021; 21(1): 321. doi: 10.1186/s12903-021-01678-x.
- Xiang H, Shen J, Wheeler KK. Efficacy of Smartphone Active and Passive Virtual Reality Distraction vs Standard Care on Burn Pain Among Pediatric Patients: A Randomized Clinical Trial. JAMA Netw Open. 2021; 4(6): e2112082. doi: 10.1001/jamanetworkopen.2021.12082.
- Ustuner Top F, Kuzlu Ayyıldız T. Pain management in children during invasive procedures: A randomized clinical trial. Nurs Forum. 2021; 56(4): 816-822. doi: 10.1111/nuf.12616
- Le May S, Hupin M, Khadra C. Decreasing Pain and Fear in Medical Procedures with a Pediatric Population (DREAM): A Pilot Randomized Within-Subject Trial. Pain Manag Nurs. 2021; 22(2): 191-197. doi: 10.1016/j.pmn.2020.10.002
- Alshatrat SM, Sabarini JM, Hammouri HM. Effect of immersive virtual reality on pain in different dental procedures in children: A pilot study. Int J Paediatr Dent. 2022; 32(2): 264-272. doi: 10.1111/ipd.12851
- CustÓdio NB, Cademartori MG, Azevedo MS. Efficacy of audiovisual distraction using eyeglasses during dental care: a randomized clinical trial. Braz Oral Res. 2021; 35: e26. doi: 10.1590/1807-3107bor-2021.vol35.0026
- Osmanlliu E, Trottier ED, Bailey B. Distraction in the Emergency department using Virtual reality for INtravenous procedures in Children to Improve comfort (DEVINCI): a pilot pragmatic randomized controlled trial. CJEM. 2021; 23(1): 94-102. doi: 10.1007/s43678-020-00006-6
- Semerci R, Akgün Kostak M, Eren T. Effects of Virtual Reality on Pain During Venous Port Access in Pediatric Oncology Patients: A Randomized Controlled Study. J Pediatr Oncol Nurs. 2021; 38(2): 142-151. doi: 10.1177/1043454220975702
- Liu KY, Ninan SJ, Laitman BM. Virtual Reality as Distraction Analgesia and Anxiolysis for Pediatric Otolaryngology Procedures. Laryngoscope. 2021; 131(5): E1714-E1721. doi: 10.1002/lary.29148
- Buyuk ET, Odabasoglu E, Uzsen H. The effect of virtual reality on Children's anxiety, fear, and pain levels before circumcision. J Pediatr Urol. 2021; 17(4): 567. doi: 10.1016/j.jpurol.2021.04.008
- Ran L, Zhao N, Fan L. Application of virtual reality on non-drug behavioral management of short-term dental procedure in children. Trials. 2021; 22(1): 562. doi: 10.1186/s13063-021-05540-x
- Gold JI, SooHoo M, Laikin AM. Effect of an Immersive Virtual Reality Intervention on Pain and Anxiety Associated with Peripheral Intravenous Catheter Placement in the Pediatric Setting: A Randomized Clinical Trial. JAMA Netw Open. 2021; 4(8): e2122569. doi: 10.1001/jamanetworkopen.2021.22569
- Koç Özkan T, Polat F. The Effect of Virtual Reality and Kaleidoscope on Pain and Anxiety Levels During Venipuncture in Children. J Perianesth Nurs. 2020; 35(2): 206-211. doi: 10.1016/j.jopan.2019.08.010
- Ä°nangil D, Åendir M, Büyükyılmaz F. Efficacy of Cartoon Viewing Devices During Phlebotomy in Children: A Randomized Controlled Trial. J Perianesth Nurs. 2020; 35(4): 407-412. doi: 10.1016/j.jopan.2020.01.008
- Taylor JS, Chandler JM, Menendez M. Small surgeries, big smiles: using virtual reality to reduce the need for sedation or general anesthesia during minor surgical procedures. Pediatr Surg Int. 2021; 37(10): 1437-1445. doi: 10.1007/s00383-021-04955-6
- Garrocho-Rangel A, Ibarra-Gutiérrez E, Rosales-Bérber M. A video eyeglasses/earphones system as distracting method during dental treatment in children: A crossover randomised and controlled clinical trial. Eur J Paediatr Dent. 2018; 19(1): 74-79. doi: 10.23804/ejpd.2018.19.01.14
- Gerçeker GÖ, Binay Å, Bilsin E, et al. Effects of Virtual Reality and External Cold and Vibration on Pain in 7- to 12-Year-Old Children During Phlebotomy: A Randomized Controlled Trial. J Perianesth Nurs. 2018; 33(6): 981-989. doi: 10.1016/j.jopan.2017.12.010. PMID: 29559294.
- Eijlers R, Dierckx B, Staals LM, et al. Virtual reality exposure before elective day care surgery to reduce anxiety and pain in children: A randomised controlled trial. Eur J Anaesthesiol. 2019; 36(10): 728-737. doi: 10.1097/EJA.0000000000001059. PMID: 31356373
- Aydın AÄ°, ÖzyazıcıoÄlu N. Using a Virtual Reality Headset to Decrease Pain Felt During a Venipuncture Procedure in Children. J Perianesth Nurs. 2019; 34(6): 1215-1221. doi: 10.1016/j.jopan.2019.05.134. PMID: 31495558
- Tennant M, Youssef GJ, McGillivray J, et al. Exploring the use of Immersive Virtual Reality to enhance Psychological Well-Being in Pediatric Oncology: A pilot randomized controlled trial. Oncol Nurs. 2020; 48: 101804. doi: 10.1016/j.ejon.2020.101804. PMID: 32949941
- Arman N, Tarakci E, Tarakci D, et al. Effects of Video Games-Based Task-Oriented Activity Training (Xbox 360 Kinect) on Activity Performance and Participation in Patients With Juvenile Idiopathic Arthritis: A Randomized Clinical Trial. Am J Phys Med Rehabil. 2019; 98(3): 174-181. doi: 10.1097/PHM.0000000000001001. PMID: 30020092
- Ali S, Manaloor R, Ma K. A randomized trial of robot-based distraction to reduce children's distress and pain during intravenous insertion in the emergency department. CJEM. 2021; 23(1): 85-93. doi: 10.1007/s43678-020-00023-5
- Lee-Krueger RCW, Pearson JR, Spencer A, et al. Children's Pain During IV Induction: A Randomized-Controlled Trial With the MEDi® Robot. J Pediatr Psychol. 2021; 46(8): 991-1000. doi: 10.1093/jpepsy/jsab028. PMID: 33764470.
- Inan G, Inal S. The Impact of 3 Different Distraction Techniques on the Pain and Anxiety Levels of Children During Venipuncture: A Clinical Trial. Clin J Pain. 2019; 35(2): 140-147. doi: 10.1097/AJP.0000000000000666
- Guinot F, Mercadé M, Oprysnyk L. Comparison of active versus passive audiovisual distraction tools on children's behaviour, anxiety and pain in paediatric dentistry: a randomised crossover clinical trial. Eur J Paediatr Dent. 2021; 22(3): 230-236. doi: 10.23804/ejpd.2021.22.03.10
- Oliveira NC, Santos JL, Linhares MB. Audiovisual distraction for pain relief in paediatric iN-PATients: A crossover study. Eur J Pain. 2017; 21(1): 178-187. doi: 10.1002/ejp.915
- van der Heijden MJE, Mevius H, van der Heijde N. Children Listening to Music or Watching Cartoons During ER Procedures: A RCT. J Pediatr Psychol. 2019; 44(10): 1151-1162. doi: 10.1093/jpepsy/jsz066
- Cheraghi F, Kalili A, Soltanian A. A Comparison of the Effect of Visual and Auditory Distractions on Physiological Indicators and Pain of Burn Dressing Change Among 6-12-Year-Oldchildren: A Clinical Trial Study. J Pediatr Nurs. 2021; 58: e81-e86. doi: 10.1016/j.pedn.2021.01.011.
- Song JS, Chung HC, Sohn S. Effects of psychological behaviour management programme on dental fear and anxiety in children: A randomised controlled clinical trial. Eur J Paediatr Dent. 2020; 21(4): 287-291. doi: 10.23804/ejpd.2020.21.04.6
- Bulut M, Küçük Alemdar D, Bulut A. The Effect of Music Therapy, Hand Massage, and Kaleidoscope Usage on Postoperative Nausea and Vomiting, Pain, Fear, and Stress in Children: A Randomized Controlled Trial. J Perianesth Nurs. 2020; 35(6): 649-657. doi: 10.1016/j.jopan.2020.03.013
- Susam V, Friedel M, Basile P, et al. Efficacy of the Buzzy System for pain relief during venipuncture in children: a randomized controlled trial. Acta Biomed. 2018; 89(6-S): 6-16. doi: 10.23750/abm.v89i6-S.7378
- Inal S, Kelleci M. The Effect of External Thermomechanical Stimulation and Distraction on Reducing Pain Experienced by Children During Blood Drawing. Pediatr Emerg Care. 2020; 36(2): 66-69. doi: 10.1097/PEC.0000000000001264
- Cozzi G, Crevatin F, Dri V. Distraction Using Buzzy or Handheld Computers During Venipuncture. Pediatr Emerg Care. 2021; 37(9): e512-e516. doi: 10.1097/PEC.0000000000001689
- Redfern RE, Chen JT, Sibrel S. Effects of Thermomechanical Stimulation during Vaccination on Anxiety, Pain, and Satisfaction in Pediatric Patients: A Randomized Controlled Trial. J Pediatr Nurs. 2018; 38: 1-7. doi: 10.1016/j.pedn.2017.09.009
- Binay Å, Bilsin E, Gerçeker GÖ. Comparison of the Effectiveness of Two Different Methods of Decreasing Pain During Phlebotomy in Children: A Randomized Controlled Trial. J Perianesth Nurs. 2019; 34(4): 749-756. doi: 10.1016/j.jopan.2018.11.010
- Yilmaz G, Alemdar DK. Using Buzzy, Shotblocker, and Bubble Blowing in a Pediatric Emergency Department to Reduce the Pain and Fear Caused by Intramuscular Injection: A Randomized Controlled Trial. J Emerg Nurs. 2019; 45(5): 502-511. doi: 10.1016/j.jen.2019.04.003. PMID: 31257044
- Yılmaz D, ÖzyazıcıoÄlu N, Çıtak Tunç G, et al. Efficacy of Buzzy® on pain and anxiety during catheterization in children. Pediatr Int. 2020; 62(9): 1094-1100. doi: 10.1111/ped.14257. PMID: 32311184.
- Bourdier S, Khelif N, Velasquez M, et al. Cold Vibration (Buzzy) Versus Anesthetic Patch (EMLA) for Pain Prevention During Cannulation in Children: A Randomized Trial. Pediatr Emerg Care. 2021; 37(2): 86-91. doi: 10.1097/PEC.0000000000001867. PMID: 31181022.
- Sivri Bilgen B, Balcı S. The Effect on Pain of Buzzy® and ShotBlocker® during the Administration of Intramuscular Injections to Children: A Randomized Controlled Trial. J Korean Acad Nurs. 2019; 49(4): 486-494. doi: 10.4040/jkan.2019.49.4.486. PMID: 31477677.
- Canbulat Sahiner N, Turkmen AS, Acikgoz A, et al. Effectiveness of Two Different Methods for Pain Reduction During Insulin Injection in Children with Type 1 Diabetes: Buzzy and ShotBlocker. Worldviews Evid Based Nurs. 2018; 15(6): 464-470. doi: 10.1111/wvn.12325. PMID: 30307692.
- Küçük Alemdar D, Yaman AktaÅ Y. The Use of the Buzzy, Jet Lidokaine, Bubble-blowing and Aromatherapy for Reducing Pediatric Pain, Stress and Fear Associated with Phlebotomy. J Pediatr Nurs. 2019; 45: e64-e72. doi: 10.1016/j.pedn.2019.01.010. PMID: 30711327.
- Ueki S, Matsunaka E, Takao K, et al. The effectiveness of vibratory stimulation in reducing pain in children receiving vaccine injection: A randomized controlled trial. Vaccine. 2021; 39(15): 2080-2087. doi: 10.1016/j.vaccine.2021.03.013. PMID: 33744043.
- Sapçi E, Bilsin Kocamaz E, Gungormus Z. Effects of applying external cold and vibration to children during vaccination on pain, fear and anxiety. Complement Ther Med. 2021; 58: 102688. doi: 10.1016/j.ctim.2021.102688. PMID: 33640458.
- Alanazi KJ, Pani S, AlGhanim N. Efficacy of external cold and a vibrating device in reducing discomfort of dental injections in children: A split mouth randomised crossover study. Eur Arch Paediatr Dent. 2019; 20(2): 79-84. doi: 10.1007/s40368-018-0399-8. PMID: 30519955.
- Bilsin E, GüngörmüÅ Z, GüngörmüÅ M. The Effıcacy of External Cooling and Vibration on Decreasing the Pain of Local Anesthesia Injections During Dental Treatment in Children: A Randomized Controlled Study. J Perianesth Nurs. 2020; 35(1): 44-47. doi: 10.1016/j.jopan.2019.06.007. PMID: 31564620.
- Zhang XH, Cui CL, Lee KK. A specially designed medical screen for children suffering from burns: A randomized trial of a distraction-type therapy. Burns. 2021; 47(5): 1137-1145. doi: 10.1016/j.burns.2020.05.018
- ErdoÄan Ç, Turan T, Pınar B. The effect of maternal voice for procedural pain in paediatric intensive care unit: A randomised controlled trial. Intensive Crit Care Nurs. 2020; 56: 102767. doi: 10.1016/j.iccn.2019.102767
- Semerci R, Akgün Kostak M. The Efficacy of Distraction Cards and Kaleidoscope for Reducing Pain During Phlebotomy: A Randomized Controlled Trial. J Perianesth Nurs. 2020; 35(4): 397-402. doi: 10.1016/j.jopan.2020.02.003
- Burns-Nader S, Joe L, Pinion K. Computer tablet distraction reduces pain and anxiety in pediatric burn patients undergoing hydrotherapy: A randomized trial. Burns. 2017; 43(6): 1203-1211. doi: 10.1016/j.burns.2017.02.015
- Kuo HC, Pan HH, Creedy DK, et al. Distraction-Based Interventions for Children Undergoing Venipuncture Procedures: A Randomized Controlled Study. Clin Nurs Res. 2018; 27(4): 467-482. doi: 10.1177/1054773816686262. PMID: 28038497.
- Grabinski ZG, Boscamp NS, Zuckerman WA. Efficacy of Distraction for Reducing Pain and Distress Associated with Venipuncture in the Pediatric Posttransplant Population: A Randomized Controlled Trial. Pediatr Emerg Care. 2022; 38(2): e811-e815. doi: 10.1097/PEC.0000000000002458
- Arıkan A, Esenay FI. Active and Passive Distraction Interventions in a Pediatric Emergency Department to Reduce the Pain and Anxiety During Venous Blood Sampling: A Randomized Clinical Trial. J Emerg Nurs. 2020; 46(6): 779-790. doi: 10.1016/j.jen.2020.05.004
- Zhang XH, Cui CL, Ren JJ. A randomized trial of a distraction-type intervention to assist in managing dressing changes for children experienced burns. J Adv Nurs. 2020; 76(3): 878-887. doi: 10.1111/jan.14278
- Alanazi KJ, Pani S, AlGhanim N. Efficacy of external cold and a vibrating device in reducing discomfort of dental injections in children: A split mouth randomised crossover study. Eur Arch Paediatr Dent. 2019; 20(2): 79-84. doi: 10.1007/s40368-018-0399-8. PMID: 30519955.
- Bilsin E, GüngörmüÅ Z, GüngörmüÅ M. The Effıcacy of External Cooling and Vibration on Decreasing the Pain of Local Anesthesia Injections During Dental Treatment in Children: A Randomized Controlled Study. J Perianesth Nurs. 2020; 35(1): 44-47. doi: 10.1016/j.jopan.2019.06.007. PMID: 31564620.
- Bergomi P, Scudeller L, Pintaldi S, et al. Efficacy of Non-pharmacological Methods of Pain Management in Children Undergoing Venipuncture in a Pediatric Outpatient Clinic: A Randomized Controlled Trial of Audiovisual Distraction and External Cold and Vibration. J Pediatr Nurs. 2018; 42: e66-e72. doi: 10.1016/j.pedn.2018.04.011. PMID: 29728296.
- García-Aracil N, Ramos-Pichardo JD, Castejón-de la Encina ME. Effectiveness of non-pharmacological measures for reducing pain and fear in children during venipuncture in the emergency department: a vibrating cold devices versus distraction. Emergencias. 2018; 30(3): 182-185. PMID: 29687673
- Chan E, Hovenden M, Ramage E, et al. Virtual Reality for Pediatric Needle Procedural Pain: Two Randomized Clinical Trials. J Pediatr. 2019; 209: 160-167. doi: 10.1016/j.jpeds.2019.02.034. PMID: 31047650.
- Dumoulin S, Bouchard S, Ellis J. A Randomized Controlled Trial on the Use of Virtual Reality for Needle-Related Procedures in Children and Adolescents in the Emergency Department. Games Health J. 2019; 8(4): 285-293. doi: 10.1089/g4h.2018.0111
- Delgado A, Ok SM, Ho D, et al. Evaluation of children's pain expression and behavior using audio visual distraction. Clin Exp Dent Res. 2021; 7(5): 795-802. doi: 10.1002/cre2.407. PMID: 33622030; PMCID: PMC8543459.
- Kumari S, Bahuguna R, Garg N, et al. Immersive and Non-Immersive Virtual Reality Distraction on Pain Perception to Intraoral Injections. J Clin Pediatr Dent. 2021; 45(6): 389-394. doi: 10.17796/1053-4625-45.6.5. PMID: 34996111.
- Newell A, Keane J, McGuire BE. Interactive Versus Passive Distraction and Parent Psychoeducation as Pain Management Techniques During Pediatric Venepuncture: A Randomized Controlled Trial. Clin J Pain. 2018; 34(11): 1008-1016. doi: 10.1097/AJP.0000000000000628
- Molleman J, Tielemans JF, Braam MJI. Distraction as a simple and effective method to reduce pain during local anesthesia: A randomized controlled trial. J Plast Reconstr Aesthet Surg. 2019; 72(12): 1979-1985. doi: 10.1016/j.bjps.2019.07.023.
- Longobardi C, Prino LE, Fabris MA, et al. Soap bubbles as a distraction technique in the management of pain, anxiety, and fear in children at the paediatric emergency room: A pilot study. Child Care Health Dev. 2019; 45(2): 300-305. doi: 10.1111/cch.12633. PMID: 30466144.
- Semerci R, Kocaaslan EN, Akgün Kostak M. Reduction of pain during intravenous cannulation in children: Buzzy application. Agri. 2020; 32(4): 177-185. doi: 10.14744/agri.2020.02223
- Jenkins N, Orsini F, Elia S. Minimising Immunisation Pain of childhood vaccines: The MIP pilot study. J Paediatr Child Health. 2021; 57(3): 376-382. doi: 10.1111/jpc.15229
- Ali S, Sivakumar M, Beran T. Study protocol for a randomised controlled trial of humanoid robot-based distraction for venipuncture pain in children. BMJ Open. 2018; 8(12): e023366. doi: 10.1136/bmjopen-2018-023366
- Goldman RD, Behboudi A. Virtual reality for intravenous placement in the emergency department-a randomized controlled trial. Eur J Pediatr. 2021; 180(3): 725-731. doi: 10.1007/s00431-020-03771-9
- Wong CL, Li CK, Chan CWH. Virtual Reality Intervention Targeting Pain and Anxiety Among Pediatric Cancer Patients Undergoing Peripheral Intravenous Cannulation: A Randomized Controlled Trial. Cancer Nurs. 2021; 44(6): 435-442. doi: 10.1097/NCC.0000000000000844
- Schlechter AK, Whitaker W, Iyer S. Virtual reality distraction during pediatric intravenous line placement in the emergency department: A prospective randomized comparison study. Am J Emerg Med. 2021; 44: 296-299. doi: 10.1016/j.ajem.2020.04.009
- Litwin SP, Nguyen C, Hundert A. Virtual Reality to Reduce Procedural Pain During IV Insertion in the Pediatric Emergency Department: A Pilot Randomized Controlled Trial. Clin J Pain. 2021; 37(2): 94-101. doi: 10.1097/AJP.0000000000000894
- Lee HN, Bae W, Park JW. Virtual reality environment using a dome screen for procedural pain in young children during intravenous placement: A pilot randomized controlled trial. PLoS One. 2021; 16(8): e0256489. doi: 10.1371/journal.pone.0256489
- Clerc PGB, Arneja JS, Zwimpfer CM. A Randomized Controlled Trial of Virtual Reality in Awake Minor Pediatric Plastic Surgery Procedures. Plast Reconstr Surg. 2021; 148(2): 400-408. doi: 10.1097/PRS.0000000000008196
- Wang Y, Chu LY, Wang SS. Preoperative video distraction alleviates separation anxiety and improves induction compliance of preschool children: a randomized controlled clinical trial. Zhonghua Yi Xue Za Zhi. 2021; 101(26): 2066-2070. doi: 10.3760/cma.j.cn112137-20201224-03458
- Trost MJ, Chrysilla G, Gold JI. Socially-Assistive Robots Using Empathy to Reduce Pain and Distress during Peripheral IV Placement in Children. Pain Res Manag. 2020; 2020: 7935215. doi: 10.1155/2020/7935215
- Jibb LA, Birnie KA, Nathan PC. Using the MEDiPORT humanoid robot to reduce procedural pain and distress in children with cancer: A pilot randomized controlled trial. Pediatr Blood Cancer. 2018; 65(9): e27242. doi: 10.1002/pbc.27242
- Bagattoni S, D'Alessandro G, Sadotti A. Effects of audiovisual distraction in children with special healthcare needs during dental restorations: a randomized crossover clinical trial. Int J Paediatr Dent. 2018; 28(1): 111-120. doi: 10.1111/ipd.12304
- Durak H, Uysal G. The Effect of Cartoon Watching and Distraction Card on Physiologic Parameters and Fear Levels During Inhalation Therapy in Children: A Randomized Controlled Study. J Trop Pediatr. 2021; 67(1): fmab018. doi: 10.1093/tropej/fmab018
- Riddell RP, O'Neill MC, Campbell L. Featured Article: The ABCDs of Pain Management: A Double-Blind Randomized Controlled Trial Examining the Impact of a Brief Educational Video on Infants' and Toddlers' Pain Scores and Parent Soothing Behavior. J Pediatr Psychol. 2018; 43(3): 224-233. doi: 10.1093/jpepsy/jsx122
- Taddio A, Coldham J, Logeman C. Feasibility of implementation of CARD™ for school-based immunizations in Calgary, Alberta: a cluster trial. BMC Public Health. 2021; 21(1): 260. doi: 10.1186/s12889-021-10247-4
- Gupta N, Gupta H, Gupta P. Evaluation of the Role of Music as a Nonpharmacological Technique in Management of Child Patients. J Contemp Dent Pract. 2017; 18(3): 194-197.
- Wang YL, Gao HX, Wang JS. Immersive virtual reality as analgesia for women during hysterosalpingography: study protocol for a randomized controlled trial. Trials. 2020; 21(1): 102. doi: 10.1186/s13063-019-4023-y
- Khadra C, Ballard A, Paquin D. Effects of a projector-based hybrid virtual reality on pain in young children with burn injuries during hydrotherapy sessions: A within-subject randomized crossover trial. Burns. 2020; 46(7): 1571-1584. doi: 10.1016/j.burns.2020.04.006
- Jenkins BN, Granger DA, Roemer RJ. Emotion regulation and positive affect in the context of salivary alpha-amylase response to pain in children with cancer. Pediatr Blood Cancer. 2018; 65(6): e26973. doi: 10.1002/pbc.26973
- Chartrand J, Tourigny J, MacCormick J. The effect of an educational pre-operative DVD on parents' and children's outcomes after a same-day surgery: a randomized controlled trial. J Adv Nurs. 2017; 73(3): 599-611. doi: 10.1111/jan.13161
- Burton KLO, Morrow AM, Beswick BV. The Feasibility of Using the BrightHearts Biofeedback-Assisted Relaxation Application for the Management of Pediatric Procedural Pain: A Pilot Study. Pain Pract. 2018; 18(8): 979-987. doi: 10.1111/papr.12696
- Sola C, Lefauconnier A, Bringuier S. Childhood preoperative anxiolysis: Is sedation and distraction better than either alone? A prospective randomized study. Paediatr Anaesth. 2017; 27(8): 827-834. doi: 10.1111/pan.13180
- Yildirim M, Koroglu E, Yucel C. The effect of hospital clown nurse on children's compliance to burn dressing change. Burns. 2019; 45(1): 190-198. doi: 0.1016/j.burns.2018.08.033
- Rodriguez ST, Jang O, Hernandez JM. Varying screen size for passive video distraction during induction of anesthesia in low-risk children: A pilot randomized controlled trial. Paediatr Anaesth. 2019; 29(6): 648-655. doi: 10.1111/pan.13636
- Kim EJ, Kim YO, Shim KW. Effects of Tranexamic Acid Based on its Population Pharmacokinetics in Pediatric Patients Undergoing Distraction Osteogenesis for Craniosynostosis: Rotational Thromboelastometry (ROTEM TM) Analysis. Int J Med Sci. 2018; 15(8): 788-795. doi: 10.7150/ijms.25008
- Bahrololoomi Z, Sadeghiyeh T, Rezaei M. The Effect of Breathing Exercise Using Bubble Blower on Anxiety and Pain during Inferior Alveolar Nerve Block in Children Aged 7 to 10 Years: A Crossover Randomized Clinical Trial. Pain Res Manag. 2022; 2022: 7817267. doi: 10.1155/2022/7817267
- Cumino DO, Vieira JE, Lima LC. Smartphone-based behavioural intervention alleviates children's anxiety during anaesthesia induction: A randomised controlled trial. Eur J Anaesthesiol. 2017; 34(3): 169-175. doi: 10.1097/EJA.0000000000000589
- Atzori B, Vagnoli L, Graziani D, et al. An Exploratory Study on the Effectiveness of Virtual Reality Analgesia for Children and Adolescents with Kidney Diseases Undergoing Venipuncture. Int J Environ Res Public Health. 2022; 19(4): 2291. doi: 10.3390/ijerph19042291
- Hu ZC, Li XB, Feng ZH. Modified pedicle screw placement at the fracture level for treatment of thoracolumbar burst fractures: a study protocol of a randomised controlled trial. BMJ Open. 2019; 9(1): e024110. doi: 10.1136/bmjopen-2018-024110
- Padminee K, Hemalatha R, Shankar P. Effectiveness of biofeedback relaxation and audio-visual distraction on dental anxiety among 7- to 12-year-old children while administering local anaesthesia: A randomized clinical trial. Int J Paediatr Dent. 2022; 32(1): 31-40. doi: 10.1111/ipd.12787
- Karaca TN, Cevik Guner U. The Effect of Music-Moving Toys to Reduce Fear and Anxiety in Preschool Children Undergoing Intravenous Insertion in a Pediatric Emergency Department: A Randomized Clinical Trial. J Emerg Nurs. 2022; 48(1): 32-44. doi: 10.1016/j.jen.2021.10.004
- Richey AE, Khoury M, Segovia NA. Use of Bedside Entertainment and Relaxation Theater (BERT) to Reduce Fear and Anxiety Associated with Outpatient Procedures in Pediatric Orthopaedics. J Pediatr Orthop. 2022; 42(1): 30-34. doi: 10.1097/BPO.0000000000002005
- Özalp Gerçeker G, Ayar D, Özdemir EZ, et al. Effects of virtual reality on pain, fear and anxiety during blood draw in children aged 5-12 years old: A randomised controlled study. J Clin Nurs. 2020; 29(7-8): 1151-1161. doi: 10.1111/jocn.15173. PMID: 31889358
- Gold JI, Mahrer NE. Is Virtual Reality Ready for Prime Time in the Medical Space? A Randomized Control Trial of Pediatric Virtual Reality for Acute Procedural Pain Management. J Pediatr Psychol. 2018; 43(3): 266-275. doi: 10.1093/jpepsy/jsx129. PMID: 29053848
- Hemphill S, Rodriguez S, Wang E, et al. Virtual Reality Augments Movement During Physical Therapy: A Pragmatic Randomized Trial. Am J Phys Med Rehabil. 2022; 101(3): 229-236. doi: 10.1097/PHM.0000000000001779. PMID: 33935153
- Caruso TJ, George A, Menendez M, et al. Virtual reality during pediatric vascular access: A pragmatic, prospective randomized, controlled trial. Paediatr Anaesth. 2020; 30(2): 116-123. doi: 10.1111/pan.13778. PMID: 31785015
- Agrawal AK, Robertson S, Litwin L, et al. Virtual reality as complementary pain therapy in hospitalized patients with sickle cell disease. Pediatr Blood Cancer. 2019; 66(2): e27525. doi: 10.1002/pbc.27525. PMID: 30362236
- Drouin S, McGrath JJ. Blood pressure and pain sensitivity in children and adolescents. Psychophysiology. 2013; 50(6): 513-20. doi: 10.1111/psyp.12036. PMID: 23517306
- Roberts J, Fenton G, Barnard M. Developing effective therapeutic relationships with children, young people and their families. Nurs Child Young People. 2015; 27(4): 30-5; doi: 10.7748/ncyp.27.4.30.e566. PMID: 25959488
- Oliver JA, Oliver LA, Aggarwal N, et al. Ambulatory Pain Management in the Pediatric Patient Population. Curr Pain Headache Rep. 2022; 26(1): 15-23. doi: 10.1007/s11916-022-00999-y. PMID: 35129824.
- Holak A, Czapla M, ZieliÅska M. Pre-Hospital Pain Management in Children with Injuries: A Retrospective Cohort Study. J Clin Med. 2021; 10(14): 3056.
- Lee JH, Espinera AR, Chen D, et al. Neonatal inflammatory pain and systemic inflammatory responses as possible environmental factors in the development of autism spectrum disorder of juvenile rats. J Neuroinflammation. 2016; 13(1): 109. doi: 10.1186/s12974-016-0575-x. PMID: 27184741