
Pain Management during Surgery for Spontaneous Abortion in Early Pregnancy: Paracervical Block
Toshiyuki Kakinuma
Center for Human Reproduction, Department of Obstetrics and Gynecology, International University of Health and Welfare Hospital, Japan
Abstract
The World Health Organization (WHO) recommends using vacuum aspiration as a surgical treatment for spontaneous and surgical abortion in early pregnancy. They also state that dilatation and curettage (D & C) should be avoided from the perspective of safety and effectiveness and to prevent the risk of endometrial injury as it can cause thinning of the endometrium and Asherman syndrome. Maintaining a good endometrial environment is important for improving the chance of pregnancy. Manual vacuum aspiration (MVA) was developed in the 1970s. For spontaneous abortion in the first trimester, MVA reduces the risk of endometrial injury, leading to less intra- and postoperative pain and simplification of anesthesia during surgical treatment for spontaneous abortion. The WHO recommends administering standard pain relief during surgical treatment for medication-induced and spontaneous abortion but does not recommend using routine general anesthesia during MVA and D & C procedures. At our hospital, we perform MVA alone under local anesthesia using a paracervical block for the surgical treatment for spontaneous abortion in early pregnancy, and the safety and effectiveness of this has been previously reported. Here, we will describe the pain management strategy used at our hospital for spontaneous abortion in early pregnancy using MVA.
Introduction
The guidelines from the World Health Organization (WHO) and the International Federation of Gynecology and Obstetrics (FIGO) recommend manual vacuum aspiration (MVA) as the surgical treatment for spontaneous and surgical abortion in early pregnancy and state that dilatation and curettage (D & C) should be avoided to ensure safety and effectiveness and avoid the risk of endometrial injury in particular1. D & C can lead to thinning of the endometrium and Asherman syndrome. In Japan, D & C with general anesthesia has been performed for a long time. Harvey Karman developed a small flexible cannula with a syringe while developing MVA, and this procedure gained popularity in the 1990s. In Japan, a manual vacuum aspirator (Women's MVA system) was approved in 2015 and can now be used in routine clinical practice. MVA enables treatment to be resumed early without undergoing infertility treatment again. Maintaining a good endometrial environment is considered an important factor in improving the chances of pregnancy. In addition, early pregnancy abortion surgery with MVA, which reduces the risk of endometrial damage, leads to less pain during and after surgery, allowing anesthesia during abortion surgery to be simplified. The WHO recommends that analgesics should be given as standard when performing medical and surgical abortions but does not recommend aspiration or routine general anesthesia for D&C1. In our hospital, we performed MVA alone under local anesthesia using a paracervical block as a surgical treatment for early pregnancy miscarriage and reported its efficacy and safety2.
We will introduce pain management in early pregnancy miscarriage using MVA at our hospital. Simplification of anesthesia in terms of endometrial protection by MVA.
In a study examining endometrial protection, Gilman-Barber et al. surveyed the state of Asherman syndrome onset in 1,580 patients who had undergone treatment for spontaneous abortion in early pregnancy, and they reported that while the onset of Asherman syndrome was observed in electric vacuum aspiration and D & C, it was not observed in MVA3. Furthermore, D & C is a risk factor for adenomyosis uteri4; however, in a report examining the incidence of adenomyosis uteri according to the procedure used for prior surgical management of spontaneous abortion, adenomyosis uteri was significantly more common in D & C than in MVA5. The idea that the endometrium needs to be of a certain thickness to establish pregnancy is widely accepted, and endometrial growth is an important factor for establishing implantation and pregnancy. Upon examining the thickness of the endometrium and the rate of prior D & C, Azumaguchi et al. reported an inverse proportion and suggested that D & C is a major cause of endometrial thinning6. In a case study of the endometrial thickness before and after MVA for spontaneous abortion, no thinning of the endometrium observed7.
MVA can be performed without curettage, and the plastic cannula used is flexible with moderate hardness; thus, there is little chance of injury to the basal layer of the endometrium; this helps prevent Asherman syndrome, endometrium thinning, and adenomyosis uteri onset. Therefore, from the perspective of endometrial protection, MVA is useful for the surgical treatment of spontaneous abortion.
Surgical treatment of spontaneous abortion in early pregnancy by MVA requires a shorter operative duration than conventional D & C. Moreover, as a thin cannula is used, surgery can be performed with slight cervical dilatation. Using a thin cannula reduces the risk of endometrial injury, which therefore leads to less intra- and postoperative pain and enables the simplification of anesthesia procedures during surgery.
Intraoperative pain management for MVA
The WHO has clearly stated that standard analgesics should be administered to all women who undergo medication-induced and surgical abortions; however, they do not recommend administering routine general anesthesia during vacuum aspiration and D & C procedures.1 Furthermore, in the guideline of the American College of Obstetricians and Gynecologists, it is noted that the surgical management of spontaneous abortion by vacuum aspiration can be performed under local anesthesia. In North America, MVA performed under local anesthesia has gained popularity8.
The uterine cervix is controlled by nerves that accompany the uterine arteries at the 3 o’clock and 9 o’clock positions, whereas the uterine fundus is controlled by nerves that accompany the uterine ligaments at the 5 o’clock and 7 o’clock positions. Therefore, it is imperative to perform local anesthesia with this positional relationship in mind. In patients with a large uterine cervix, the procedure might sometimes be easier by using an intracervical block.
For the paracervical and intracervical block, a colposcope is inserted into the vagina and the vagina and uterine cervix are disinfected. Next, a 23 G cathelin needle with xylocaine 1 % injection syringe (10 mL) is used for the local injection. For the paracervical block, 2.5 mL of 1 % lidocaine is injected at a depth of 15 to 20 mm at each site, including the 2, 4, 8, and 10 o’clock positions to avoid injury to the uterine arteries. In contrast, in the intracervical block, a puncture is performed at a depth of 15 to 20 mm with an injection needle in the cervical canal at the 2, 4, 8, and 10 o’clock positions, and 5 mL of 1 % lidocaine is injected into each site (Figure 1). When local injection into the cervical canal is difficult, uterovaginal forceps are used; however, in such instances, for pain management, it is important to use the uterovaginal forceps after injecting 2 mL of the xylocaine 1 % injection syringe (10 mL) locally into the area where the uterovaginal forceps will be applied. Also, the plunger is pulled once during administration to confirm the absence of backflow to avoid intravascular mis-administration. Moreover, in the event of surgery for spontaneous abortion, as practitioners, we must never forget to eliminate patient anxiety by always talking to the patient and providing nursing intervention such as ‘touching care’.
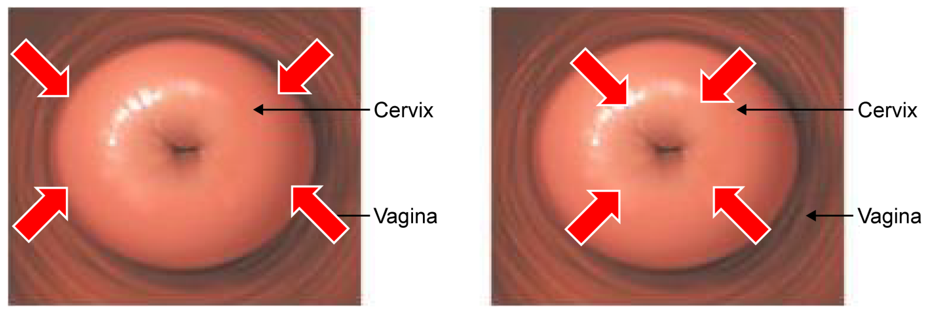
Figure 1: Local anesthesia administration site for paracervical and intracervical blocks.
Paracervical canal blocks were used; using a 23-gage cattelan needle, 2.5 mL of 1% xylocaine was locally injected to a depth of 15–20 mm at four different clock positions: 2, 4, 8, and 10 o’clock. In patients with a large uterine cervix, the procedure might sometimes be made easier with an intracervical block.
At our hospital, we perform local anesthesia using a paracervical block for pain management of early spontaneous abortion by MVA. We have performed MVA under local anesthesia in 166 cases by December 2020. Per the patient’s wishes and if needed, concurrent intravenous injection of an analgesic or sedative is considered; however, their use is not required to date. In terms of controlling intraoperative pain, pain control is good compared with MVA performed under conventional intravenous anesthesia (15 mg of pentazocine and 1–1.5 mg/kg of propofol 1%). High treatment satisfaction can be achieved (Figures 2 and 3) with no complications with this treatment2.
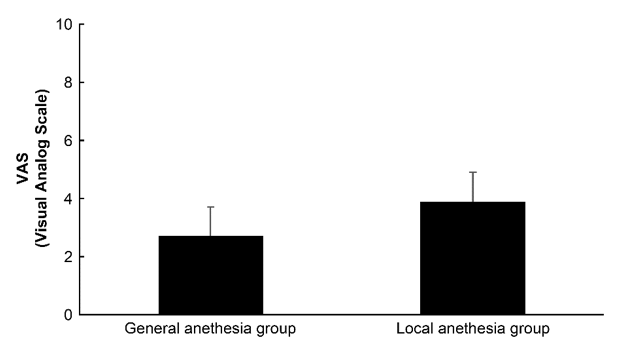
Figure 2: Manual vacuum aspiration pain scale according to the administered anesthesia procedure (cited from reference 2).
No significant differences were noted between the two groups in terms of the visual analog scale scores for pain.
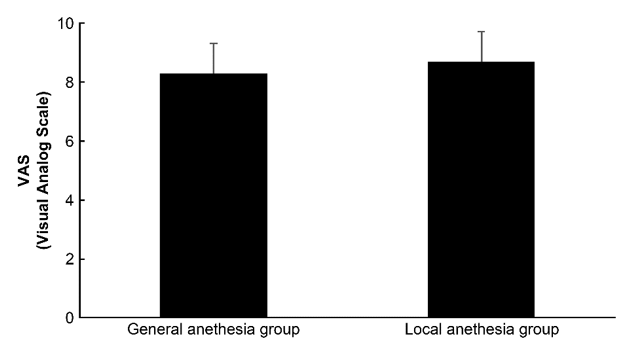
Figure 3: Patient satisfaction with manual vacuum aspiration according to the administered anesthesia procedure (cited from reference 2).
No significant differences were noted between the two groups in terms of the visual analog scale scores for treatment satisfaction.
Furthermore, avoiding general anesthesia is advantageous in that a large reduction in cost can be expected, the time for recovery after anesthesia administration is less, equipment and staff to administer general anesthesia are not required, and the risk of complications due to anesthesia is reduced9.
Although using local anesthesia has many advantages, the risk of local anesthetic toxicity should always be considered. Care must be taken to prevent overdose or intravenous mis-administration of local anesthetics. We performed surgery with the venous path ensured by attaching an electrocardiogram, blood pressure monitor, and pulse oximeter. Furthermore, there are systems in place, including an oxygen bag and mask and emergency medications that allow taking appropriate measures, including cardiopulmonary resuscitation in the event of the patient’s condition worsening.
Conclusion
Maintaining a good endometrial environment is considered an important factor in improving the chance of pregnancy. In preconception care, the establishment of minimally invasive surgical management of spontaneous abortion in early pregnancy that does not lead to requiring new infertility treatments and aimed toward subsequent pregnancy is needed. The surgical treatment of early spontaneous abortion, as recommended by the WHO and FIGO, is effective and safe from the perspective of endometrial protection. Furthermore, it can be performed under local anesthesia, and anesthesia administration can be simplified. In the future, the clinical importance of MVA under paracervical block is expected to increase.
List of abbreviations
FIGO : Federation of Gynecology and Obstetrics
MVA : Manual Vacuum Aspiration
WHO : World Health Organization
D & C : Dilatation and Curettage
Competing Interests
There are no competing interests to disclose.
References
- World Health Organization. Expanding health worker roles for safe abortion in the first trimester of pregnancy. 2016. Available from: https://www.who.int/reproductivehealth/publications/unsafe_abortion/health-worker-roles-safe-abortion-1st-trimester-summary/en/. Accessed 5 June 2022.
- Kakinuma T, Kakinuma K, Kaneko A, et al. Safety and efficacy of manual vacuum aspiration under local anesthesia compared to general anesthesia in the surgical management of miscarriage: a retrospective cohort study. Patient Saf Surg. 2022; 16(1): 16.
- Gilman-Barber AR, Rhone SA, Fluker MR. Curettage and Asherman's syndrome-lessons to (Re-) Learn? J Obstet Gynaecol Can. 2014; 36(11): 997-1001.
- Kishi Y, Suginami H, Kuramori R, et al. Four subtypes of adenomyosis assessed by magnetic resonance imaging and their specification. Am J Obstet Gynecol. 2012; 207(2): 114.e1-7.
- Sordia-Hernándeza LH, Guerrero-Gonzáleza G, Morales-Martíneza A, et al. Treatment for incomplete abortion with manual vacuum aspiration is related with lower prevalence of adenomyosis in women who underwent a hysterectomy. Medicina Universitaria. 2012; 14(55): 86-89.
- Azumaguchi A, Henmi H, Ohnishi H, et al. Role of dilatation and curettage performed for spontaneous or induced abortion in the etiology of endometrial thinning. J Obstet Gynaecol Res. 2017; 43(3): 523-529.
- Kakinuma T, Kakinuma K, Sakamoto Y, et al. Safety and efficacy of manual vacuum suction compared with conventional dilatation and sharp curettage and electric vacuum aspiration in surgical treatment of miscarriage: a randomized controlled trial. BMC Pregnancy Childbirth. 2020; 20(1): 695.
- O'Connell K, Jones HE, Simon M, et al.; National Abortion Federation Members. First trimester surgical abortion practices: A survey of National Abortion Federation members. Contraception. 2001; 64: 345-352.
- The American College of Obstetricians and Gynecologists Practice Bulletin no. 150. Early pregnancy loss. Obstet Gynecol. 2015; 125(5): 1258-1267.